There is hardly a fate worse than being confined to a bed. Injuries to the legs can be a source of lifelong pain or, even worse, immobility. At Ganga Hospital we have accumulated a vast experience in literally putting people back on their feet.
Recent years have shown a disconcerting spurt in road accidents and their concomitant injuries, especially involving the lower limbs. Many of those involved are young and bread earners for their families. Along with our Anaesthesia and Orthopaedic teams, the Department of Plastic and Reconstructive Microsurgery has made great strides in the art and science of limb reconstruction. Many injuries that were once considered non-salvageable, hence doomed for an amputation, are now being saved with a combination of cutting edge techniques, broad experience and sheer doggedness in pursuit of a shared goal. That to build our Nation by not letting our injured lie by the wayside.
Road traffic accidents are common in India. As the bone in the leg is superficial, when it breaks in an accident it easily tears the overlying skin. The tissues in the leg and the bones are now exposed to the dirt at the place of the accident. The patient may have a lot of bleeding. This usually settles down by itself when the limb is kept elevated. As the bones are broken even mild movements of the leg may produce severe pain. The dirt in the wounds will give rise to infection and prevent the bone from uniting unless the wound is cleaned well. Hence the patient must be shifted to hospital soon.
When the patient comes to the hospital, the patient will be resuscitated and checked whether he has any other life threatening injuries. Once that has been ruled out, X rays of the injured lower limb will be taken. The patient will be examined by a senior plastic surgeon and an orthopaedic surgeon who will then talk to the patient and his attenders about the injury, what needs to be done, the cost, time taken for the wounds to heal and for the patient to walk. If both the patient and the doctors agree to go ahead with salvage of the limb and further reconstruction, the patient is taken to the operation theatre immediately where the plastic surgeon would debride and clean the wound well under magnification and good lighting so that the wounds can heal well. The orthopaedic surgeon would then fix the bones so that the bones are in good alignment. In simple injuries we may be able to close the skin. However in severe injuries we may not be able to close the skin and would need further plastic surgical procedures to cover the skin and the fracture site so that the bone and the wounds will heal well. This may be done in the same sitting or it may be done in another operation which is usually done within the next 2 to 3 days by the plastic surgeon. After the wound heals well, the orthopaedic surgeon decides whether to continue the fixation or change the fixation to a definitive fixation.
It is preferable to bring the patient as early as you can. Patients who have injuries to the major blood vessels of the lower limb such as the femoral artery or the popliteal artery may need to be brought to the hospital urgently within 6 hours as these blood vessels provide the blood flow to the lower limb. Delay would mean that the lower limb may not be saved and may have to be amputated. Hence if you are not able to feel the pulse in the foot, the patient has to come urgently to a hospital which has both plastic surgeons or vascular surgeons who can bring back the blood flow to the distal limb and an orthopaedic surgeon who can stabilise the bones well. Even if the patient has a pulse, it is preferable to bring the patient as early as you can. It has been proved that if the wounds in the legs are cleaned well, bones are fixed early and if the wounds are covered early, the bone heals well and the patient can walk better and faster.
The structure of a lower limb consists of bone and soft tissues like skin, fat, muscles, blood vessels, tendons and nerves. In a crush injury of the lower limb, a combination of the above structures are injured. The plastic surgeon takes care of the damage to all the soft tissues namely the skin, muscles, fat, blood vessels, nerves and the tendons. Hence the role of a plastic surgeon in a major crush injury of the lower limb are:-
When a patient has a road traffic accident, a lot of mud and dirt contaminates the wounds. This minute mud and dirt can serve as a nidus for bacteria to grow and this can result in infection. The tissues surrounding the infected wounds get inflamed resulting in pain, swelling and pus discharge from the wounds. Preventing this problem is more important than treating it. This problem can be prevented by good early surgical debridement (Cleaning of wounds) by an experienced team. When a patient gets admitted, irrespective of the time, the patient is taken to the theatre. With good lighting and magnification with loupes, we carefully remove all the dirt and mud particles in order to prevent infection.

Pre OP

Radical Debridement

Flap inset
.JPG)
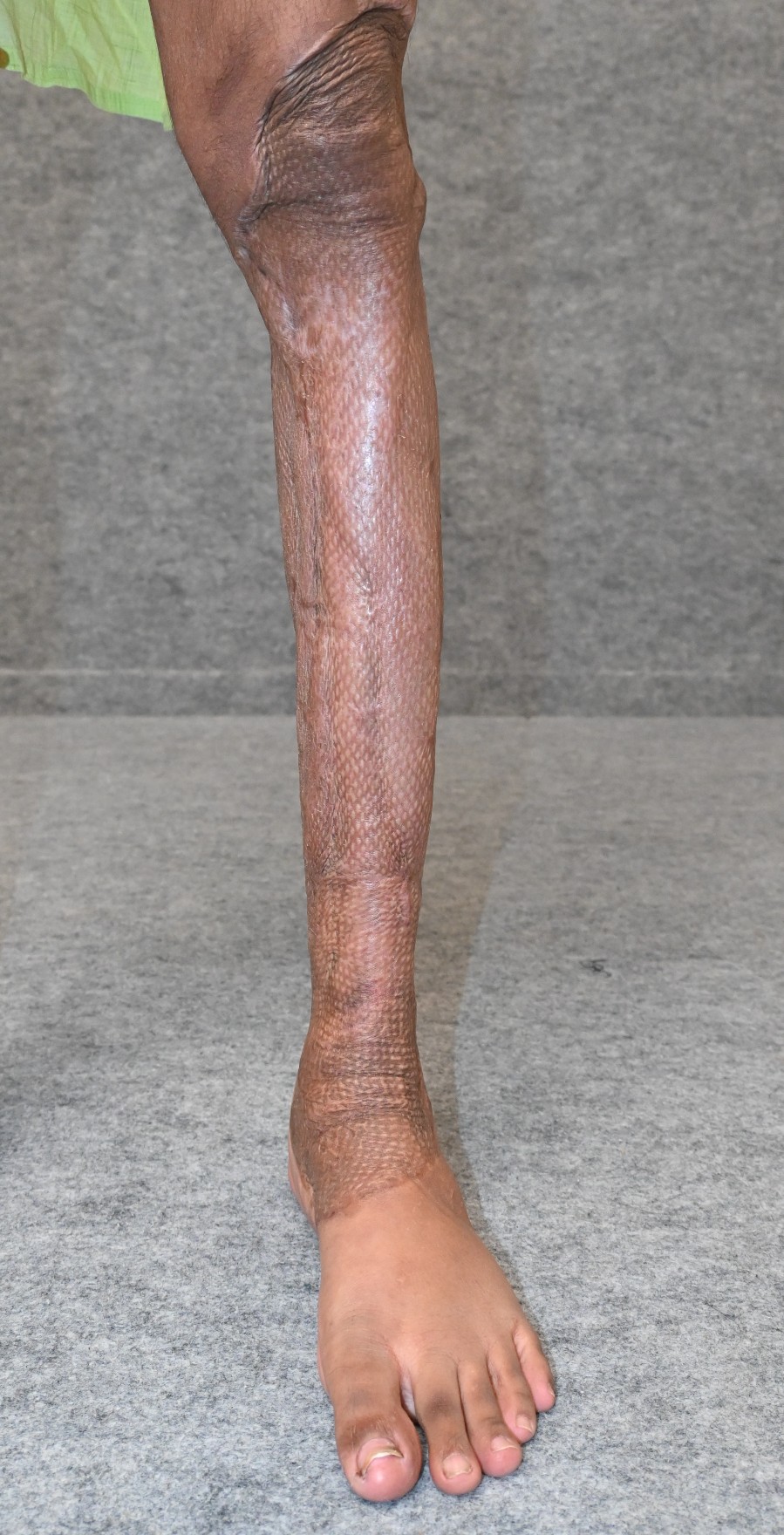
Post operative
.JPG)
Post operative
Most lower limb injuries are major crush injuries. They are best treated in a major trauma hospital where there are senior plastic surgeons, orthopaedic surgeons and anaesthesiologists. At Ganga Hospital we have senior plastic surgeons, orthopaedic surgeons and anesthesiologists who would receive the patient round the clock and would do the needful immediately. At Ganga Hospital we operate on around 1000 open fractures of the limbs every year making us one of the most experienced in tackling these injuries. The high load of injuries that we get is a testament to the trust that our patients have had on us.
Fractures to the bone of the thigh (Femur), fractures to the bone in the leg (Tibia) or dislocations of the knee can either occlude or rupture the major artery that supplies blood to the lower limb. When there is injury to major blood vessels such as the femoral artery or the popliteal artery, there is reduced or absent blood flow to the part of the limb distal to the injured site. If not tackled urgently we may not be able to save the leg and the patient may go for above knee amputation. If there is no pulse in the foot we must consider injury to these major vessels unless proved otherwise. Here time is a premium and is very important. They need to be brought to a major trauma centre. These cases are extremely challenging as this needs a very experienced team of orthopaedic surgeons, plastic surgeons and anaesthesiologists. The patient is taken to theatre immediately. Resuscitating these patients and getting them on to the table needs very experienced anaesthesiologists. The fractures are then stabilised by the orthopaedic surgeon. Then the plastic surgeon cleans the wounds, and explores for injury to the vessel. We have found that after the injured segment of the artery is removed, we have to bridge the gap with another spare vein from the leg. This is done by microsurgery where the operation is done under the microscope as very thin sutures are used to repair the blood vessels. We have also found that injury to the major artery does not occur alone and these patients almost always have soft tissue defects to cover which as plastic surgeons we do even in the primary surgery at times to cover the blood vessel. To save the limbs of these patients, this needs an experienced team which does well in every step.






Injury to the tibial nerve can result in reduced or absent sensations of the foot and can result in reduced movement of the ankle or knees. Many institutions consider this as an indication for amputation. However in our experience we have found that patients do well when this nerve is repaired and we take all efforts to save the limb. Repair of this nerve has to be done with fine sutures under the microscope to get a good result. If there is a gap in the nerve we bridge the gap in the nerve with a less important nerve to give sensations to the feet.
Skin cover is very essential for the wounds to heal well. Only when the overlying soft tissue heals will the underlying fracture heal. The choice of skin cover depends on the part of the leg that is exposed. If a muscle or fat is exposed, this can be covered with a skin graft. However when a bone, tendon, joint or orthopaedic implants are exposed, then the area has to be covered with a flap.
The outer half of skin is harvested from an area distant from the wound. This is called a skin graft. This is then sutured to a defect over the leg which has good blood supply to the base of the wound. The skin grows back from the place where the graft is taken from.


Presenting Picture


Post Debridement Picture


SSG



If the base of the wound does not have an adequate blood supply, tissues which have a good blood supply is used to cover the defect. This tissues with good blood supply is called as a flap.
Usually the tissues with good blood supply are got from tissues nearby. They are called as pedicle flaps. However, due to paucity of adjacent tissues, tissues can be harvested from a distant place along with it’s blood supply and are connected to the blood vessels near the defect and this is called as a free flap.
Tendons are cord like structures at the end of the muscles which help to move the toes and the ankles. Repairing them would help us to make them move the toes and the ankles. After repairing the tendons they need to undergo physiotherapy and rehabilitation.
Our primary aim is that every patient should have an independent painless independent walking within a timeframe and cost that the patient can afford. We try to salvage most of the limbs that we can. However, if the limb is crushed beyond redemption we tend to offer amputation as it might be the best way that the patient can walk fast. In certain cases where the patient has a major crush injury with bone and soft tissue loss, treatment and rehabilitation of the patient might involve multiple surgeries, prolonged duration and increased cost. In those cases we explain to the patient the pros and cons of salvage of the limb well and help them make the right decision. In certain cases, especially in patients with multiple comorbid problems amputation might be a good choice as the patients may walk early with good prosthesis tha are available now.


Chairman
Chairman, Division of Plastic Surgery, Hand Surgery, Reconstructive Microsurgery and Burns








