



What is a Cancer?
What is the thyroid gland?
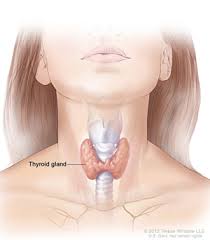
- The thyroid is a small butterfly-shaped gland present in front of the neck. It produces a hormone called thyroxine which affects the growth, development and function of almost all the cells in the body.
- The thyroid is a small butterfly-shaped gland present in front of the neck. It produces a hormone called thyroxine which affects the growth, development and function of almost all the cells in the body.