



What is a Cancer?
What are salivary glands?
What are the signs and symptoms of a salivary gland tumour?
How common are Salivary gland Neoplasms?
How can we diagnose salivary gland neoplasms?
What are the risk factors of salivary gland Neoplasms?
What are the surgeries performed for salivary gland tumours?
What are the complications of salivary gland surgeries?
Although we make several efforts to reduce the complications, there can be some complications such as
- Facial nerve palsy
The facial nerve is a nerve responsible for the proper functioning of the muscles of expression of the face. While operating on malignant tumours of the parotid gland, the facial nerve might need to be sacrificed to clear the cancer cells properly. In these cases, the facial nerve is reconstructed with nerve grafts. In benign tumours of the parotid gland, the part of the parotid gland superficial to the facial nerve is removed. Facial nerve damage in these cases is overcome by good surgical expertise, nerve monitoring in selected instances, Ontable nerve grafts with microscopes and advanced plastic surgical techniques. Even though the facial nerve may not be damaged during surgery, the facial nerve may not work for a few days to weeks as the dissection is done close to the nerve. In these cases, the nerve recovers with time.
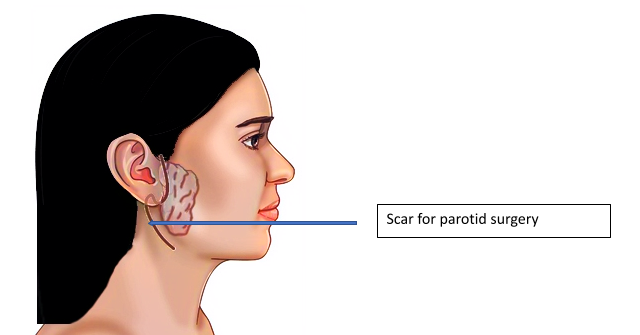
- Scar in the face.
The scar is hidden around the ear and then followed into the neck to be not very obvious. They usually heal very well. If they heal with hypertrophic scars, we use multiple techniques like scar massage, compression, LASER to heal them well.
- Bleeding & Infection
These are rare complications that can happen after any surgery. They settle with time.
- Sweating over parotid area while eating)- Frey’s Syndrome-
It occurs in approximately 10% of the patient. This happens as the nerves overlying the parotid are cut. Most cases settle on its own with medications and some injections. Rarely they need surgery.