OPD Days Tuesday, Thursday, Saturday 2 PM to 5 PM
We are open for emergency 24 X 7
Diabetic foot care is one of the most ignored aspects of diabetes care in India. Due to social, religious, and economic compulsions, many people walk barefoot. Poverty and lack of education lead to usage of inappropriate footwear and late presentation of foot lesions. Many non-medically qualified persons are interfering in the treatment of diseases, including diabetes. Patients also try home remedies before visiting their physicians. It estimated that 90% of diabetic patients in India do not see a specialist in their lifetime. Problem is further worsened by a delay in accessing healthcare due to patient approaching informal care providers and alternative medicine prescribers.
There’s a lot to manage if you have diabetes: checking your blood sugar, making healthy food, finding time to be active, taking medicines, going to doctor’s appointments. With all that, your feet might be the last thing on your mind. Foot problems are common in people with diabetes. You might be afraid you’ll lose a toe, foot, or leg to diabetes, or know someone who has, but you can lower your chances of having diabetes-related foot problems by taking care of your feet every day.
India is set to become the diabetes capital of the world with a projected 109 million individuals with diabetes by 2035. India ranks second (after China) with more than 66.8 million diabetics in the age group of 20-70. The prevalence of Diabetes in India is 8.6% and, as of 2013, more than 1 million Indians die each year due to diabetes related causes. Diabetic Foot (DF) is one of the most common complications for admissions imposing tremendous medical and financial burden on our healthcare system. The lifetime risk of a person with diabetes having a foot ulcer could be as high as 25% and is the commonest reason for hospitalization of diabetic patients (about 30%) and absorbs about 20% of the total health-care costs, more than all other diabetic complications. The prevalence of foot ulcers in diabetics attending a centre managing diabetic foot (both indoor and outdoor setup) in India is 3%. Foot ulcers among outpatient and inpatient diabetics attending hospitals in rural India was found to be 10.4%. Peripheral vascular disease (PVD) occurs in about 3.2% diabetics below 50 years of age and rises to 55% in those above 80 years of age. 15% of those with diabetes for a decade suffer from diabetic foot, where as it increases to almost 50% by another decade.
Approximately, 85% of non-traumatic lower limb amputations are seen in patients with prior history of diabetic foot ulcer. Each year, more than 1 million people with diabetes lose at least a part of their leg due to diabetic foot. It shows that every 20 seconds a limb is lost in the world somewhere. In India, though recent population based data is not available, it is estimated that approximately 45,000 legs are amputated every year in India. The vast majority (75%) of these are probably preventable because the amputation often results from an infected neuropathic foot. More than half of all foot ulcers become infected, requiring hospitalization, while 20% of infections result in amputation. After a major amputation, 50% of people will have the other limb amputated within two years’ time. People with a history of diabetic foot ulcer have a 40% greater 10-year death rate than people with diabetes alone.
For treating a simple and complex diabetic foot ulcer in low Income countries like India can be equivalent to 5.7 years of average annual income. However, pain and suffering, loss of mobility, even life-long dependence on others and limitations imposed by the change of role is incalculable. The management of diabetic foot requires a holistic and rigorous approach without which there will be high levels of relapse, morbidity and even mortality. The expenditure on care for amputation has two fold burden on patient as well as health care system with requirement for surgery, postoperative care followed by rehabilitation and the need for adaptations to home and prostheses fitting. However, prevention is clearly more cost effective than cure in diabetic foot management.
Multi-disciplinary approach
Diabetic Foot Ulcers are wounds that occur in the feet of persons with diabetes mellitus. About 15% of all diabetics develop a foot ulcer. Foot ulcers are treatable and curable the earlier they are brought to appropriate medical attention. Treating a foot ulcer is all about healing an ulcer without recurrence.
At Ganga Hospital we have created an entire ecosystem to treat the entire spectrum of Diabetic Foot ulcers right from the simplest to the most complicated wound requiring microsurgical reconstruction. Our philosophy at Ganga Hospital is to address the wound at an early stage by suitable therapy to ensure that there is recurrence free healing. Such a philosophy helps us to prevent wound complications like infection which may lead to loss of the limb.
For the unfortunate few who require a major amputation, we have established in collaboration with Otto Bock (one of the largest prosthesis makers in the world) a centre that provides prosthetic limbs made with cutting edge technology.
At Ganga Hospital all medical professionals involved in the care of diabetic foot patients, the Diabetologist, Plastic Surgeon, Orthopedic Surgeon, Vascular Surgeon, Intensive care specialist, Anesthesiologist, Physiotherapist and Footwear specialist collaborate under one roof to provide wholesome care.
Diabetic patients are fragile patients with many other life-threatening problems like cardiac, renal problems. Giving anaesthesia to them is riskier than the surgery itself. Hence our anaesthesia team specialises in regional and nerve blocks which are safer in fragile diabetic patients.
If you are a person with Diabetes Mellitus then the following signs may help you identify that your foot needs care. (* - Signs that mandate an urgent visit to the hospital)
Over time, diabetes may cause nerve damage, also called diabetic neuropathy, that can cause tingling and pain, and can make you lose feeling in your feet. When you lose feeling in your feet, you may not feel a pebble inside your sock or a blister on your foot, which can lead to cuts and sores. Cuts and sores can become infected.
Diabetes also can lower the amount of blood flow in your feet. Not having enough blood flowing to your legs and feet can make it hard for a sore or an infection to heal. Sometimes, a bad infection never heals. The infection might lead to gangrene.
Gangrene and foot ulcers that do not get better with treatment can lead to an amputation of your toe, foot, or part of your leg. A surgeon may perform an amputation to prevent a bad infection from spreading to the rest of your body, and to save your life. Good foot care is very important to prevent serious infections and gangrene.
Although rare, nerve damage from diabetes can lead to changes in the shape of your feet, such as Charcot’s foot. Charcot’s foot may start with redness, warmth, and swelling. Later, bones in your feet and toes can shift or break, which can cause your feet to have an odd shape, such as a “rocker bottom.”
People with diabetes are at increased risk of peripheral arterial disease and neuropathy, as well as having a higher risk of developing infections and decreased ability to clear infections. Therefore, people with diabetes are prone to frequent and often severe foot problems and a relatively high risk of infection, gangrene and amputation.
Some people with nerve damage have numbness, tingling, or pain, but others have no symptoms. Nerve damage can also lower your ability to feel pain, heat, or cold.
Living without pain sounds pretty good, but it comes at a high cost. Pain is the body’s way of telling you something’s wrong so you can take care of yourself. If you don’t feel pain in your feet, you may not notice a cut, blister, sore, or other problem. Small problems can become serious if they aren’t treated early.
Anyone with diabetes can develop nerve damage, but these factors increase your risk:
Keep your blood sugar in your target range as much as possible. Other good diabetes management habits can help, too:
Because of sensory deficits, there are no protective symptoms guarding against pressure and heat and so trauma can initiate the development of a leg ulcer. Absence of pain contributes to the development of Charcot foot, which further impairs the ability to sustain pressure. Motor fibre abnormalities lead to undue physical stress and to the development of further anatomical deformities (arched foot, clawing of toes), and contribute to the development of infection. When infection complicates a foot ulcer, the combination can be limb-threatening or life-threatening. Detection and surveillance of diabetic neuropathy are an essential routine part of a diabetic annual review.
A Charcot foot is a joint and bone problem with weakening of bones, fracture, acute inflammation and disorganisation of foot architecture. The Charcot foot is characterised by bone and joint degeneration which can lead to a devastating deformity. It usually presents as a hot swollen foot with or without antecedent minor trauma. Slight trauma triggers fracture of a weakened bone, which increases the load on adjacent bones, leading to gross destruction. The process is self-limiting but the persisting deformity greatly increases the risk of secondary ulceration. Suspected Charcot neuro-arthropathy of the foot is an emergency and should be treated by expert doctors. Plain X-ray may be normal and specialists may order for MRI scan. Damage and developing deformity should be limited by immobilising the foot in a castor sometimes surgery to prevent amputation.
If established charcot’s foot with an ulcer is seen, ulcer has to be healed first and then this may be followed by orthopaedic surgery for fixing your weakened and fractured bones.



Diabetic ulcerations are often one of the first signs of complications from diabetes in the lower leg. These ulcers can stem from a small wound or cut on the foot that is slow to heal. If left untreated, ulcers can become harder to treat and could lead to amputation. If discovered early and treated by a specialist, ulcers may not lead to amputation.
Diabetic foot ulcers can occur because of two main reasons - Peripheral Neuropathy (damage to the nerves that connect your feet to your spinal cord), Ischemia (reduction in blood supply to your feet or a combination of both with long standing Diabetes or Pre-Diabetes. Majority (85%) of Diabetic Foot ulcers develop in patients with good blood supply to the feet. That means that most of these cases are easily curable with proper focussed treatment at an early stage. Such ulcers are called Neuropathic Ulcers. The loss of nerve function causes these feet to develop abnormalities and deformities that cause excessive pressure on the sole of the foot. These areas of excessive pressure then develop areas of skin thickening called calluses. The callus which starts off to protect the skin gradually increases in size and thickness over time in response to the increased pressure. Soon it turns big enough to act like a hard stone and by itself increases the pressure on the underlying skin (by about 30%) thereby hastening skin breakdown resulting in ulceration. Once an ulcer forms the continuing excessive pressure on the area prevents the ulcer from healing and it becomes a non-healing ulcer resistant to any form of conservative management like dressings and ointment application.
Other complications contributing to the onset of ulceration include poor vision, limited joint mobility, and the consequences of cardiovascular and cerebrovascular disease. However, the most common precipitant is accidental trauma, especially from ill-fitting footwear. Reduced blood supply compounds the problem. Once the skin is broken, many processes contribute to defective healing, including bacterial infection, tissue ischaemia, continuing trauma, and poor management.

Walking on a shard of glass

Spreading Infection due to the un-recognized wound

Ischemic Gangrene of the Great toe

Ischemic Gangrene of the entire foot
The only treatment that can give consistent, predictable and recurrence free healing is appropriate offloading surgery
Following the natural history of Diabetic foot ulcers - neuropathic ulcers cause problems mainly because of infection. The ulcer acts as a portal of entry to pathogenic bacteria which then cause a localized or spreading infection. The spread of infection follows anatomical tissue planes.
Localized Infection: The infection may initially start as a local warmth and redness with swelling of the surrounding tissues which if left unchecked can progress in to an abscess. Abscess formation is usually indicated by the presence of fever, a tense painful foot. If it involves the bone then it causes osteomyelitis and bony destruction.
Abscess & Gangrene: The abscess can then start spreading in localized tissue planes throughout the foot resulting in spreading gangrene.
Sepsis: Once the long tendons or other planes are infected the infection then rapidly spreads to the leg and also into the blood stream and can cause the patient to become very sick resulting in sepsis.
Following the natural history of Diabetic foot ulcers - neuropathic ulcers cause problems mainly because of infection. The ulcer acts as a portal of entry to pathogenic bacteria which then cause a localized or spreading infection. The spread of infection follows anatomical tissue planes.
Localized Infection: The infection may initially start as a local warmth and redness with swelling of the surrounding tissues which if left unchecked can progress in to an abscess. Abscess formation is usually indicated by the presence of fever, a tense painful foot. If it involves the bone then it causes osteomyelitis and bony destruction.
Abscess & Gangrene: The abscess can then start spreading in localized tissue planes throughout the foot resulting in spreading gangrene.
Sepsis: Once the long tendons or other planes are infected the infection then rapidly spreads to the leg and also into the blood stream and can cause the patient to become very sick resulting in sepsis.

Localized infection of the Great toe

Abscess complicating a 5th metatarsal head ulcer

Spreading infection in the leg
Foot ulcers in people with diabetes have a high risk of necessitating amputation. Ulcer recurrence rates are high; however, appropriate education for patients, regular surveillance, the provision of post-healing footwear and regular foot care can reduce rates of re-ulceration. Early detection and effective management of diabetic foot ulcers can reduce complications, including preventable amputations and possible mortality
Risk factors for foot ulceration include peripheral arterial disease, peripheral neuropathy, previous amputation, previous ulceration, presence of callus, joint deformity, problems with vision and/or mobility, and male sex. Risk factors for peripheral arterial disease include smoking, hypertension and hypercholesterolaemia.
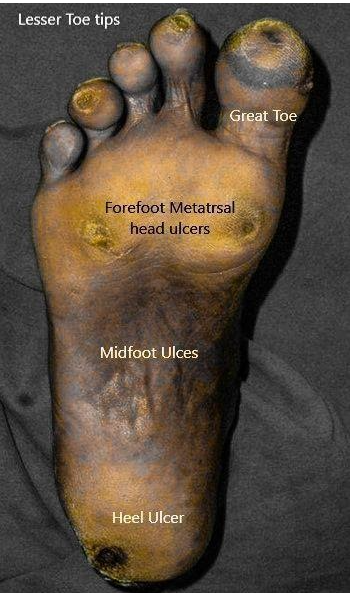
Neuropathic diabetic foot ulcers commonly occur on the sole of the foot in Diabetic patients. They can occur mainly in 5 specific areas of importance in the frequency shown below.
The 5 specific areas of diabetic foot ulcers are:
The other common problems which can cause infection in the feet of person with diabetes include –
Mortality rates after diabetic foot ulceration and amputation are high, with up to 70% of people dying within five years of having an amputation and around 50% dying within five years of developing a diabetic foot ulcer. This high mortality rate is believed to be associated with cardiovascular disease, and emphasises the importance of good diabetic and cardiovascular risk management. Only way to reduce the mortality is being healthy, prevent ulcers and be walking on the feet.
Yes, there are many. We follow the Ganga Hospital Staging of Diabetic Foot Proper treatment of an ulcer requires for the ulcer to be staged properly and then treated as per the stage. All previous staging systems have relied upon main three factors to stage the wound
The main purpose of most of the staging systems have been to take into account the above three factors and use them to communicate risk of amputation or to predict outcome
The most common staging systems are the Meggitt and Wagner staging and University of Texas staging systems. Both of the above use the above variables in different combinations to stage a wound into up to 16 possible stages and both of the above systems do not incorporate Charcot’s neuro-osteoarthropathy as a risk factor and do not serve as a guide to the type of therapy needed for a particular ulcer amongst the gamut of presentations.
The type and complexity of therapy needs to be escalated as the complexity and complications of an ulcerated foot. Early problems can be managed with conservative methods that like Callus debridement, moisturizers and good footwear. Once the ulcer develops and is not responsive to any conservative method the patient must undergo preventive surgery to correct the responsible pathomechanics and allow the ulcer to heal. Some patients may present with signs of localized invasive infection such as cellulitis, abscess formation of osteomyelitis. These patients require debridement (preferably under tourniquet) and if there is a resultant skin of soft tissue loss; they need to undergo reconstructive surgery in the form of Grafts or Flaps. Rarely the patient may present with a neglected foot with rapidly spreading infection and gangrene and sepsis which poses a threat to life. Such patients require a major amputation without wasting further time.
Some patients present with early signs of Ischemia or Charcot Osteoarthropathy are grouped with stage 3 patients. Such feet can usually be saved by directing the patient to the appropriate tertiary care centre. Patients with gross ischemic gangrene or advanced Charcot neuro-osteoarthropathy with extensive loss of bone are candidates for early amputation and are classified together with the previous stage 4 patients
The Ganga Hospital Staging system of Diabetic Foot ulcers is a simple staging system which develops up on the older classification systems, is treatment oriented and is highly suitable for day to day practice at the General physician level onwards. It clearly specifies which patients require surgery and also recommends the type of surgery that may be required and the specialist who would best suit the situation. It also indicates the need for involvement of other specialities when needed.
Staging your foot gives an idea about:
As far as treatment is considered,
stage 1 : requires preventive podiatry.
Stage 2 : requires, surgical offloading procedures.
Stage 3 : requires control of infection by surgery and antibiotics, another major surgery to correct the damage suffered by your foot to reasonable level.
Stage 4 : most likely will land up with major amputation.
Annually for people who are at low risk. Frequently (for example, every 3-6 months) for people who are at moderate risk. More frequently (for example, every 1-2 months) for people who are at high risk, if there is no immediate concern. Very frequently (for example, every 1-2 weeks) for people who are at moderate/ high risk, if there is immediate concern. We may advise for more frequent reassessments for people who are at moderate or high risk and for people who are unable to check their own feet.
Ulcers that occur on the ball of the toes are called forefoot ulcers. They typically occur underneath the heads of metatarsal bones which are the bones that connect the midfoot with the toes. The metatarsal heads are important for efficient walking (propulsive gait). They are aligned in such a way that all five metatarsal heads equally bear weight during standing. However, in people with neuropathy the metatarsals get mal-aligned due to loss of intrinsic muscle support and hence one metatarsal may become relatively more prominent during walking than the others causing a localized ulcer under the forefoot. In some people this mal-alignment of the metatarsals may co-exist with a dynamic or structural equinus contracture of the ankle (a condition which causes the ankle to stay in relative plantar flexion throughout the stance phase of walking) and this causes the forefoot to become additionally stressed. Patients with forefoot ulcers need to be evaluated to find out all the reasons for causation of the ulcer and then appropriately treat them so that the chance of a recurrence of the ulcer is minimized.
The various forms of therapy include
The advantage of surgical offloading therapy for diabetic foot ulcers includes faster rates of healing, lower recurrence rates and reduced chances of infective complication.

Ulcers in the tip of minor Toes

Tip ulcers in minor toes occurs due to clawing or plantar bending of the tip of toes. Due to clawing, pulp does not come in contact during strike and lift off of the gait cycle, instead tip of the toes hammers into the surface while walking. Usually clawing is due to hyperactivity or shortening of flexor tendons. Flexor tenotomy either percutaneous or open will release the flexor tendons and correct the clawing, again getting pulp contact on the gait cycle.
The ulcers in tip of toes will heal with dressings and complete bed rest. Though non surgical offloading will effectively heal the wound, the results will be temporary as the biomechanical factors are still deranged. Hence when patient starts weight bearing the ulcer as a rule recurs even after foot wear modification
The bones of the toes are just beneath the tip of your toes. If the infection spreads to the bones or the tendons, it is difficult to treat them. Spreading to the bone may require removal of the bone. Spread of infection to the tendons will ease and hasten the spread of infection to larger part of foot. Moreover there may be gangrene or blackening or decay of your toes, which requires removal of your toe.
Flexor tenotomy is usually advised for the ulcers in tip of the toes.
Flexor tenotomy means cutting the flexor tendons to the toes.
This procedure is usually advised for toe tip ulcers and patients who have crowded toes leading to intertrigo – fungal infection between toes.
The surgery may be done through percutaneous approach – piercing a needle and cutting the tendon or by open approach – incising the skin and expose the tendons and cut them. Percutaneous procedure could take 5-10 mins for each toes. The open approach will take 15 mins for each toes.
Usually both the procedures are done in local anaesthesia and sometimes open flexor tenotomy may require regional anaesthesia
Post operatively, non-bulky dressings will be done. Dressings can be changed by patient at home after gentle soap and water wash daily. He/She can resume activities after 24 hours in case of percutaneous tenotomy. However, open tenotomy patients should avoid weight bearing on the foot operated till their sutures are removed. They will have to visit doctors once in a week till their wounds heal.
In percutaneous flexor tenotomy, there is literally no wound. So after 24 hours, one can start doing essential jobs. In case of open flexor tenotomy, they need to take rest till stitches are removed. Removing stitches will take upto two weeks.
Preventive podiatry is the method of choice to treat the pre-ulcer foot (Callosity stage). It consists of shaving of the callus, application of emollient creams, proper cutting of nails, wearing appropriate custom-made prescription footwear (available in-house) and compression garments. These methods need to be followed even after the ulcer is healed to keep the feet soft and supple and prevent any future ulcers
Footwear for Diabetes patients is used to redistribute the pressure from areas of excessive force to the entire foot. This results in lowering of peak pressure in the prominent ares and helps to prevent ulcer formation. Diabetic footwear widely available and of varying quality and technology. However, people with “at risk” pre – ulcer foot the best that today’s technology has to offer is a custom-made prescription footwear. At Ganga Hospital we have tied up with “Diastride” to provide the best quality diabetic footwear at competitive rates to ensure the best for our patients. We have the entire range of footwear to to suit all pockets and ensure that the patient gets the best for what he pays.
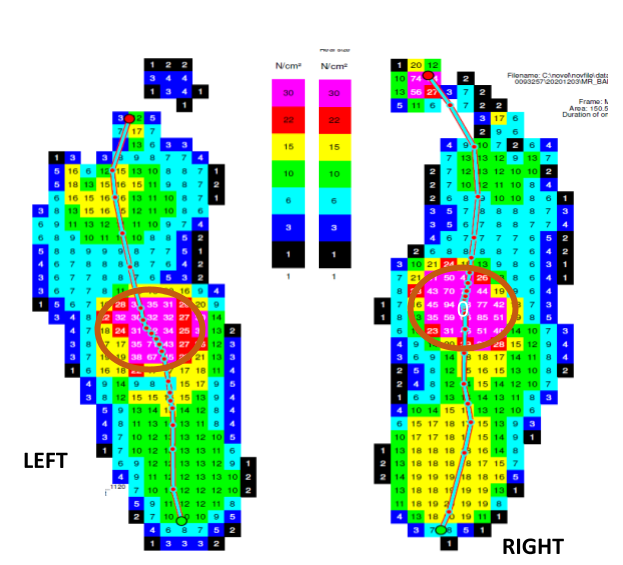
Pedobarography, otherwise known as force plate testing is a device used to measure the ground reaction forces produced by the foot on walking. This is achieved by using the latest force plate equipment which is connected to a computer which analyses the data and presents it in a visual form. This test requires the patient to walk bare-footed on a track in which the force plate is embedded.
The data is used by the surgeon to understand the pattern of the patient’s gait and the way different forces are transmitted during walking. It helps plan the appropriate surgical correction.
The data from force plate testing is also used to design and manufacture appropriate customized prescription footwear. It helps to design the shape of the footwear insole and to provide the foam of appropriate density asper the pressures transmitted by the patient’s foot.
Amputation commonly refers to the removal of any extremity or external part of the body.
Amputation of the lower limb is a life-saving procedure. It is done in patients in whom the lower limb has become dead due to infection or loss of blood supply. The dead tissues release toxic substances into the circulation, which can cause the failure of the critical organs like heart, liver and kidney in diabetic patients. Prolonged exposure to these toxins can cause irreversible damage to these organs resulting in multi-organ failure and death. It is also done in some cases with soft tissue defects or bony defects which prevent ambulation and reconstruction is complicated or not possible
The most commonly done amputations in diabetes are removal of the toes, part of the foot (Transmetatarsal amputation) or the entire foot at a level just below the knee (Below knee amputation) and rarely removal of the leg at the mid or lower thigh (Above knee amputation). Of these amputations only, the Below knee and Above knee amputations need fitting of artificial limbs for further walking. Toe amputations or partial foot amputations do not need any sort of artificial limb for walking.
No. Modern prosthesis technology has made it possible for even the frailest of persons to walk independently using artificial lower limbs. It is necessary to wear a good quality prosthesis, and this must be fit at a dedicated prosthetic centre with full-time prosthetists available for proper scientific training and support. It is essential that the patient has a good experience with the prosthesis from day one so that they feel confident and motivated to continue using the prosthesis. In our experience, we have many older adults who now lead a good quality of life after a major amputation and fitting of good artificial limbs.
On an average, it takes about 2 weeks for a stump to heal after surgery. However, the stump needs some time for maturation before it becomes ready to fit an artificial limb. During this waiting period, the amputee is taught muscle strengthening exercises and undergoes compression therapy to reduce the swelling in the stump.
Artificial limbs in diabetic patients are usually fit at about four weeks after the stump wounds heal or about 6 weeks after the operation. However, a few patients who are very weak and have poor heart and lung function may require some more time before they are strong enough to walk with artificial limbs
All patients who have been amputation and fitted with artificial limbs have the potential to achieve their pre-amputation activity levels. All that they require is a proper professional training, support and motivation from family members. Those patients who have a will and desire to walk, jog or run will not be hindered from achieving their wish due to an amputation. This has been made possible due to technologically advanced, lightweight and robust materials used in the manufacture of the modern prosthesis. Hence it is essential to choose a good prosthesis with good pre and post fitting support and service.

A Callus is a thickened area of the outermost layer of skin (Epidermis) that if formed as a response of that part of the body to repetitive mechanical trauma such as pressure, shear and friction
Calluses develop as a protective mechanism. When a part of the skin (commonly foot and hands) is subjected to repetitive forces the epidermis thickens due to accumulation of keratotic cells. This helps that part of the skin to withstand these forces better
Though calluses develop as a protective response of the skin to mechanical trauma they turn deleterious in a few people, especially, in those without adequate sensation in their feet. As dead cells accumulate in the callus it becomes harder in nature. Slowly it becomes so hard that this callus starts to act like a stone under the foot. When it reaches this stage, it increases the pressure on the skin under the callus by about 30% which hastening its breakdown resulting in an ulcer[1]. In effect the callus which was formed to protect the underlying skin ends up hastening its damage. Hence it is advisable for people with insensate feet to get their feet checked for calluses and get them removed at regular intervals.
As Soon as possible. Studies have shown that for a diabetic person the risk of getting an ulcer is 11 times higher when they have an untreated callus[2]. A callus is a pre-ulcerative change and hence it is advisable to get professional help at a dedicated centre once you develop a callus. In people with diabetic foot disease it is said that TIME = TISSUE. Hence the earlier you get medical attention, greater is the chance of preventive tissue loss.
A callus is usually managed by application of keratolytic creams or mechanically by shaving of the callus till normal skin. However, the advantages of getting your callus checked at a dedicated foot care centre is that doctors will be able to identify the specific reason for callus formation and treat the underlying cause (deformity or stiffness of joints) earlier in the course of the problem. A pedicure at a beauty care centre, done improperly with unsterile instruments and self-taught technicians who do not understand the vulnerable and tender nature of the diabetic foot is an assault on the foot which may lead to undesirable consequences.
No. Callus removal is an out-patient (OP) procedure which can be done in the surgeon’s office. It does not require any anesthesia or admission as an inpatient as it is a painless procedure which involves removal of dead cells only.
Most patients are allowed to walk immediately after a callus removal but a small subset of patients who have had a removal of a black coloured callus (due to bleeding under the callus which indicates the formation of a sub-callus ulcer) may require to rest the foot to allow the wound to heal before they are given customized footwear and allowed to walk.
Yes. You can go back to work as soon as you are allowed to walk.
Yes. As no anesthesia is required you can drive back home. Those with a black callus are advised to rest the foot for a few days to allow it to recuperate before they resume their normal activities. However, it must be noted that all diabetics with callus must wear customized prescription footwear at all times when they are one their feet (both within and outside of their homes).

Cellulitis means the inflammation of the subcutaneous cellulite (fatty) tissues. The most common reason is a bacterial infection of the fatty tissues below the skin.
Cellulitis presents with pain, swelling and redness of the affected area. The patient may or may not have an associated fever. The patient usually mistakes the pain for a sprain or muscle pull and massages the area with oil or a pain balm which may worsen the problem by causing the infection to spread to newer areas.
Cellulitis mostly develops in immunocompromised patients like those with Diabetes or other causes of low immunity. Many patients are actually found to be diabetic for the first time during the course of treatment for a cellulitis episode. In these susceptible patients a small inoculum of bacteria in the skin and subcutaneous fatty tissues due to a trivial trauma or other factors like a nail infection or cracks in the skin of the feet can cause these bacteria to rapidly spread within the cellulite tissues both by direct invasion and spread by lymphatic tissues.
It is advisable to get admitted into the hospital in the event of being diagnosed with cellulitis of the limbs. The first and foremost requirement of management is complete rest and elevation of the affected limb. Antibiotics preferably as injection through the veins are more effective than if taken by mouth. The affected limb needs to be reviewed often by a doctor to check for progression (in which case treatment needs to be escalated) or resolution. Management of associated contributory factors like Diabetes and skin diseases are best addressed as an inpatient.
On diagnosis the problem is managed with broad spectrum antibiotics preferably through the intravenous (veins) route. Strict bed rest with limb elevation helps resolution of the problem. Despite adequate measures a minority of patients who do not respond adequately may reqire surgical decompression and drainage of the involved area. This pre-emptive surgery prevents the progression of the problem into a Necrotising Soft Tissue Infection (NSTI) which can lead to extensive skin and soft tissue gangrene necessitating extensive plastic surgery for wound healing
In the presence of a predisposing condition like diabetes the risk of recurrence of cellulitis always exists. However, if the patient strictly follows medical advice then the chances of a recurrence can be minimized. Keeping a low threshold for seeking medical help can help the patient to be identified at an early stage of the problem and this increases the chances of avoiding unnecessary surgery. The patient needs to keep their feet protected, moisturized and free from edema by wearing appropriate footwear at all times, strictly using moisturizing creams and by the regular use of elastic compression garments which are provided to them after the resolution of the first episode of cellulitis.
The time to be off work depends on the severity of the disease with which the patient presents to the hospital. Early cellulitis without systemic symptoms can usually be contained within a week but those patients presenting with severe Necrotising Soft Tissue Infection (NSTI) may require about 3 to 6 months to regain their previous levels of activity. Hence it is always better to catch the problem early.

Corn Foot (Heloma / Clavus) is a painful condition of the foot that results from the formation of hardened areas of skin usually on the sole of the foot.
Corns are formed due to the increased thickness of the outermost layer of the skin, the epidermis in response to repetitive mechanical trauma such as friction, pressure or shear forces
Early corns and calluses (corn like lesions without the central keratotic core or plug) can be treated with creams containing keratolytic agents such as Salicylic acid in varying concentrations. They are available both as prescription drugs and over the counter preparations. Their effectiveness however varies from patient to patient.
Corns usually arise from focal mechanical trauma , in response to which the outer layer of the skin, the epidermis, becomes thicker nad ultimately turns into a corn. Good footwear helps reduce the trauma to the foot and thereby helps to reduce the formation of new corns.
Custom made footwear is the best that todays technology has for the deformed and insensate foot such as the feet of diabetic patients. Offloading of pressure does not only mean taking off pressure from the affected area but it also means that the redistribution of that pressure evenly over other areas of the foot. Wearing customized footwear is the best way to achieve such equal redistribution of pressure
Surgery is advised intractable and painful corns unresponsive to conservative measures like Ointments and footwear change.
Surgery is usually done under local anesthesia in the operation theatre with good facilities. No surgery is minor enough to be undertaken without the best of precautions. In our hospital as a policy we perform even the simplest of procedures in the operation theatre with an experienced anaesthetist present.
Local anesthesia is usually given if it is a single corn. However, for people with multiple corns a regional anesthesia is preferred where only the involved foot and leg below the level of the knee is made to go numb by the help of a small injection in the leg itself and then operation is done.
Surgery will take about 15 minutes for a single corn to about half an hour for multiple corns. This includes the time to give anesthesia and prepare the patient.
If surgery is done under local anesthesia you can go home in a couple of hours but if regional anesthesia is used then an overnight stay is preferable as the leg take about 8 to 12 hours to recover sensation and movement.
If a simple corn excision is done then you can start walking on the affected leg in a couple of days. However, in patients in whom a flap surgery (plastic surgery) is done, walking is prohibited on the affected leg for about 2 weeks till the suture lines heal and suture removal is done. Hence working people can plan their schedule accordingly.
Pain will be present after the operation for about a day or two. During this period, you will be given pain killers to manage the pain. Rest and elevation of the operated part are simple measures that have a profound effect on reduction of pain.
People with diabetes mellitus usually have reduced pain sensation after the operation and hence tend think that there isn’t any risk by walking. However early walking can increase the chance of wound infection and reduce the speed of healing. Other than these factors diabetics do not have any increased risk or need to worry.
Corns have a moderately high risk of recurrence if the original cause of mechanical trauma is not addressed by using good footwear and keratolytic creams.
After surgery patients in whom only an excision is done and the wound left to contract and heal will have to wash the wound with a mild soap and clean water. They can then pat it dry with a clean towel and apply dressings with the provided ointment and dressing material that will be prescribed at the time of discharge.
Complicated (Stage 3) ulcers are those ulcers that have become complicated by invasive bacterial infection of the soft tissues or bone underlying the ulcer. It is a consequence of progressive deepening of the ulcer and once the underlying loose tissue planes such as tendon, bone or joint become exposed the bacteria gain access to these planes of loose tissue resistance and cause a rapidly spreading infection which if left unchecked may result in loss of the leg
Once they gain entry the bacterial multiplication is exponential. For example if bacterial cell divides into two every one hour then the total number of bacteria after the first 10 hours would be 210 (1024), after 20 hours would be 220 (1048576) and after 30 hours would be 230 (1073741824). Once this exponential growth reaches a critical number it soon overwhelms the already weak immune system of a diabetic patient resulting in a rapidly spreading infection that causes extensive gangrene of skin and soft tissue (Flesh eating disease). Hence early intervention is required to limit the spread of tissue infection often best achieved by a multipronged strategy of antibiotic usage along with surgical excision and drainage of the dead and infected tissues. It would be most apt to use the phrase Time = Tissue in this situation.
Debridement is the surgical removal of all infected and dead tissues which harbour bacteria. It also includes the drainage of pus collection. This procedure is best done in the operation theatre with appropriate and adequate anesthesia and tourniquet control to prevent blood loss. Debridement done in the bedside or out patient settings is usually inadequate and increase the risk of losing the limb by providing the patient and surgeon with a false sense of security leading to delay and loss of valuable time and tissue.
Once debridement is over the surgeon reassesses the wound bed. Depending on the exposure of critical structures such as bone, joint and tendons the type of cover is determined. If the bed exposes critical structures a flap (a piece of tissue transferred from one place to another having its own blood supply and which does not depend on the bed for its survival) is used for cover and wound healing. If no critical structures are exposed then a split skin graft usually suffices.
Resting of the affected part followed by isometric and isotonic exercises till the wound completely heals is the usual post-operative course. Once healing has taken place the patient is given appropriate footwear and allowed walk bearing weight on the affected part. Some patients may be advised to undergo a second surgery to prevent recurrence of the ulcer which caused the original problem
Patient can be made to walk without bearing weight on the affected leg with a help of a walker device (photo) as soon as two weeks following the definitive procedure. However, those who require further corrective surgery are advised to rest until the wound heals. A few patients are allowed to walk with weight bearing on the affected leg after the application of a protective plaster of Paris cast.
Amputation is usually kept as a last resort. It is done in patients with extensive gangrene, life threatening infection or in complicated ulcers with structural soft tissue and bone loss which precludes a meaningful limb reconstruction.
Diabetic Foot Ulcers are wounds that occur in the feet of persons with diabetes mellitus. About 15% of all diabetics develop a foot ulcer. Foot ulcers are treatable and curable the earlier they are brought to appropriate medical attention. Treating a foot ulcer is all about healing an ulcer without recurrence.
At Ganga Hospital we have created an entire ecosystem to treat the entire spectrum of Diabetic Foot ulcers right from the simplest to the most complicated wound requiring microsurgical reconstruction. Our philosophy at Ganga Hospital is to address the wound at an early stage by suitable therapy to ensure that there is recurrence free healing. Such a philosophy helps us to prevent wound complications like infection which may lead to loss of the limb.
For the unfortunate few who require a major amputation, we have established in collaboration with Otto Bock (one of the largest prosthesis makers in the world) a centre that provides prosthetic limbs made with cutting edge technology.
At Ganga Hospital all medical professionals involved in the care of diabetic foot patients, the Diabetologist, Plastic Surgeon, Orthopedic Surgeon, Vascular Surgeon, Intensive care specialist, Anesthesiologist, Physiotherapist and Footwear specialist collaborate under one roof to provide wholesome care.
Diabetic Foot ulcers develop due to damage to the nerves and blood vessels of the leg and foot in patients with long standing Diabetes or Pre-Diabetes. Majority (85%) of Diabetic Foot ulcers develop in patients with good blood supply to the feet. That means that most of these cases are easily curable with proper focussed treatment at an early stage. Such ulcers are called Neuropathic Ulcers. The loss of nerve function causes these feet to develop abnormalities and deformities that cause excessive pressure on the sole of the foot. These areas of excessive pressure then develop areas of skin thickening called calluses. The callus which starts off to protect the skin gradually increases in size and thickness over time in response to the increased pressure. Soon it turns big enough to act like a hard stone and by itself increases the pressure on the underlying skin (by about 30%) thereby hastening skin breakdown resulting in ulceration. Once an ulcer forms the continuing excessive pressure on the area prevents the ulcer from healing and it becomes a non-healing ulcer resistant to any form of conservative management like dressings and ointment application. The only treatment that can give consistent, predictable and recurrence free healing is appropriate offloading surgery.
Preventive podiatry is the method of choice to treat the pre-ulcer foot (Callosity stage). It consists of shaving of the callus, application of emollient creams, proper cutting of nails, wearing appropriate custom-made prescription footwear (available in-house) and compression garments. These methods need to be followed even after the ulcer is healed to keep the feet soft and supple and prevent any future ulcers
Footwear for Diabetes patients is used to redistribute the pressure from areas of excessive force to the entire foot. This results in lowering of peak pressure in the prominent ares and helps to prevent ulcer formation. Diabetic footwear widely available and of varying quality and technology. However, people with “at risk” pre – ulcer foot the best that today’s technology has to offer is a custom-made prescription footwear. At Ganga Hospital we have tied up with “Diastride” to provide the best quality diabetic footwear at competitive rates to ensure the best for our patients. We have the entire range of footwear to to suit all pockets and ensure that the patient gets the best for what he pays.
Pedobarography, otherwise known as force plate testing is a device used to measure the ground reaction forces produced by the foot on walking. This is achieved by using the latest force plate equipment which is connected to a computer which analyses the data and presents it in a visual form. This test requires the patient to walk bare-footed on a track in which the force plate is embedded.
The data is used by the surgeon to understand the pattern of the patient’s gait and the way different forces are transmitted during walking. It helps plan the appropriate surgical correction.
The data from force plate testing is also used to design and manufacture appropriate customized prescription footwear. It helps to design the shape of the footwear insole and to provide the foam of appropriate density asper the pressures transmitted by the patient’s foot.
Proper treatment of an ulcer requires for the ulcer to be staged properly and then treated as per the stage. All previous staging systems have relied upon main three factors to stage the wound
The main purpose of most of the staging systems have been to take into account the above three factors and use them to communicate risk of amputation or to predict outcome
The most common staging systems are the Meggitt and Wagner staging and University of Texas staging systems. Both of the above use the above variables in different combinations to stage a wound into up to 16 possible stages and both of the above systems do not incorporate Charcot’s neuro-osteoarthropathy as a risk factor and do not serve as a guide to the type of therapy needed for a particular ulcer amongst the gamut of presentations.
The type and complexity of therapy needs to be escalated as the complexity and complications of an ulcerated foot. Early problems can be managed with conservative methods that like Callus debridement, moisturizers and good footwear. Once the ulcer develops and is not responsive to any conservative method the patient must undergo preventive surgery to correct the responsible pathomechanics and allow the ulcer to heal. Some patients may present with signs of localized invasive infection such as cellulitis, abscess formation of osteomyelitis. These patients require debridement (preferably under tourniquet) and if there is a resultant skin of soft tissue loss; they need to undergo reconstructive surgery in the form of Grafts or Flaps. Rarely the patient may present with a neglected foot with rapidly spreading infection and gangrene and sepsis which poses a threat to life. Such patients require a major amputation without wasting further time.
Some patients present with early signs of Ischemia or Charcot Osteoarthropathy are grouped with stage 3 patients. Such feet can usually be saved by directing the patient to the appropriate tertiary care centre. Patients with gross ischemic gangrene or advanced Charcot neuro-osteoarthropathy with extensive loss of bone are candidates for early amputation and are classified together with the previous stage 4 patients
The Ganga Hospital Staging system of Diabetic Foot ulcers[2] is a simple staging system which develops up on the older classification systems, is treatment oriented and is highly suitable for day to day practice at the General physician level onwards. It clearly specifies which patients require surgery and also recommends the type of surgery that may be required and the specialist who would best suit the situation. It also indicates the need for involvement of other specialities when needed.
| Stage | Description | Wound Factors | Additional factors |
|---|---|---|---|
| 1 | Foot at risk | Callus, Loss of protective sensation | Foot pulses present (At least one), No bony pathology |
| 2 | Ulcerated Foot | Presence of ulcer, No invasive infection, Presence of bony deformitity | Foot pulses present (At least one), No bony pathology |
| 3 | Crippled Foot | Ulcer with Invasive infection (Abscess/ Osteomyelitis/ Infective Tenosynovitis) | Early Ischemia with or without minor gangrene / Active Charcot osteoarthropathy with good bone stock |
| 4 | Critical foot | Infected Ulcer with Frank Sepsis | Major Ischemic gangrene/ Active Charcot osteoarthropathy with Loss of Bone stock negating Orthopedic intervention |
Chairman
Chairman, Division of Plastic Surgery, Hand Surgery, Reconstructive Microsurgery and Burns



